 One of the major goals of parenting is the socialization of children, during which parents teach their children to cope with the stresses of life in socially appropriate ways. At certain developmental ages, (i.e. temper tantrums in toddlers or adolescent rebellion), negative and disruptive displays of behavior are fleeting and considered “normal.” When these behaviors present with greater intensity or frequency than would be expected and persist throughout childhood, they become an area of clinical concern. The term “disruptive behavior” includes temper tantrums, excessive whining or crying, demanding attention, noncompliance, defiance, aggressive acts against self or others, stealing, lying, destruction of property, and delinquency. Clinical and developmental research supports the theory that appropriate parental responses to child behaviors create a key factor in the development and maintenance of positive child behaviors. Programs designed to train parents in principles of social learning and in effective parent-child interaction and child management skills have been designed as treatments.
One of the major goals of parenting is the socialization of children, during which parents teach their children to cope with the stresses of life in socially appropriate ways. At certain developmental ages, (i.e. temper tantrums in toddlers or adolescent rebellion), negative and disruptive displays of behavior are fleeting and considered “normal.” When these behaviors present with greater intensity or frequency than would be expected and persist throughout childhood, they become an area of clinical concern. The term “disruptive behavior” includes temper tantrums, excessive whining or crying, demanding attention, noncompliance, defiance, aggressive acts against self or others, stealing, lying, destruction of property, and delinquency. Clinical and developmental research supports the theory that appropriate parental responses to child behaviors create a key factor in the development and maintenance of positive child behaviors. Programs designed to train parents in principles of social learning and in effective parent-child interaction and child management skills have been designed as treatments.
Behaviorally based parent-child interaction training programs are the most common and successful treatment approaches for disruptive behavior among young children and most parents report significant satisfaction with these programs. In addition, parent training is compatible with the current demands of mental health care delivery systems because it is cost-effective, time-limited, and empirically validated, and requires careful documentation of treatment gains.
Parent-Child Interaction Therapy (PCIT) is an evidence-based parent training program developed by Dr. Sheila Eyberg. During this approach, the therapist coaches the parent during real-time interactions with the child, most often from behind a one-way mirror utilizing a bug-in-the-ear hearing device.
Parents develop two types of skills in this approach. During the first phase of treatment, Child-Directed Interaction (CDI), parents learn to use traditional play therapy skills to enhance the parent-child relationship. CDI skills include praising, reflection, imitating, describing, being enthusiastic, and providing contingent attention. In the second phase of treatment, Parent-Directed Interaction (PDI), parents learn skills for improving child compliance and decreasing disruptive behaviors. The PDI skills include giving effective commands, praising compliance, using a structured time-out procedure for non-compliance, and establishing standing house rules. PCIT is a short-term treatment that typically requires 12 one-hour sessions, if the parents are consistent. However, progression through the treatment program is based on skill mastery, which is assessed through a standardized coding system, such that the treatment length is tailored to individual families. PCIT is concluded only when the parent masters both the CDI and PDI skills and the child’s behavior improves to be within normal limits.
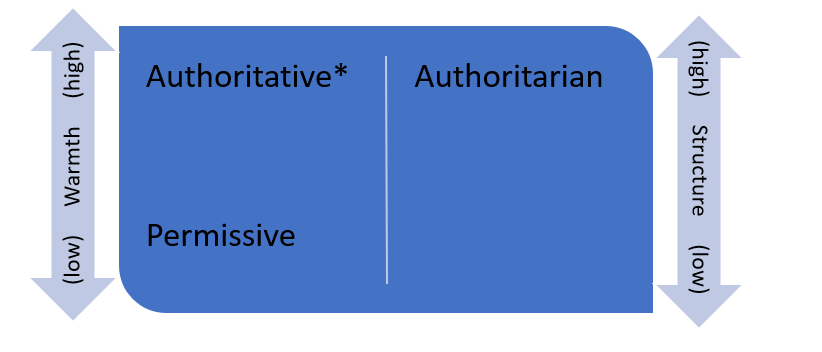
PCIT was developed from a background in operant theory, traditional child psychotherapy, and early child development. The theoretical basis for PCIT is Diana Baumrind’s work regarding parenting styles. Baumrind proposed that children have dual needs for nurturance (warmth) and for limits (structure). She described three parenting styles based on these two dimensions. Authoritarian parenting style is high in structure and low in warmth. This style typically results in children who are anxious, withdrawn, and show poor frustration tolerance. Permissive parenting is high in warmth but low in structure. This parenting style results in children with poor emotional regulation, rebelliousness and defiance, and low persistence. Authoritative parenting consists of parents who are high in both warmth and structure and this style has shown the best outcomes in children. Children raised by authoritative parents are lively and happy, self-confident, show good emotional regulation, and have good social skills.
Eyberg created PCIT with the hopes of drawing on both attachment and social learning theories to achieve authoritative parenting. The two dimensions of Baumrind’s authoritative parenting, nurturance and limit-setting mirror the two phases of PCIT. Eyberg drew heavily from attachment theory in conceptualizing the child-directed phase of treatment. For the parent-directed phase of treatment, Eyberg draws from social learning theory, which maintains that disruptive behavior is developed and maintained by parental reinforcement such as providing negative attention and allowing children to escape demands. In the parent-directed phase of treatment, parents are taught to set limits and provide consistent consequences while avoiding negative, escalating interactions with the child.
Eyberg was also heavily influenced by the two-stage operant model developed by Constance Hanf. In this model, during the first stage, parents were taught differential reinforcement, a technique during which parents give their attention to positive behavior and ignore negative behaviors. In the second stage, parents were taught to give clear directions, consistently reward compliance with praise, and provide a time-out consequence for non-compliance.
Eyberg also recognized the impact of play therapy on building a warm and safe therapeutic relationship. Eyberg found that parents could be taught traditional play therapy skills of following the child’s lead, providing undivided attention, describing play activities, reflecting and expanding upon child verbalizations, and imitation. PCIT integrates operant methods and traditional play therapy techniques within a solid developmental framework. PCIT in conducted in the context of 2-person play situations because play is the primary developmental medium through which children learn problem-solving skills and work through developmental problems. Thus, a developmental perspective is crucial in providing effective PCIT. The key features of PCIT are working with the child and parent together, direct coaching of parent-child interactions, using data to guide treatment, intervening early, targeting a range of behavioral problems, specialized space and equipment, targeting patterns of interaction rather than discrete behaviors, and having a positive, non-judgmental philosophy.
For more information on working through parent child relationship and behaviors, including telehealth options, contact us! We can help.